“The CRAB criteria for detection of multiple myeloma evaluate patients based on four parameters: hypercalcemia, renal impairment, anemia, and bone lesions. When diagnosing Black and African American patients, it's important to account for their typically lower hemoglobin levels and renal function, as these factors can influence the assessment.”
Cesar Rodriguez, MD
Associate Professor
Icahn School of Medicine at Mount Sinai
New York, NY
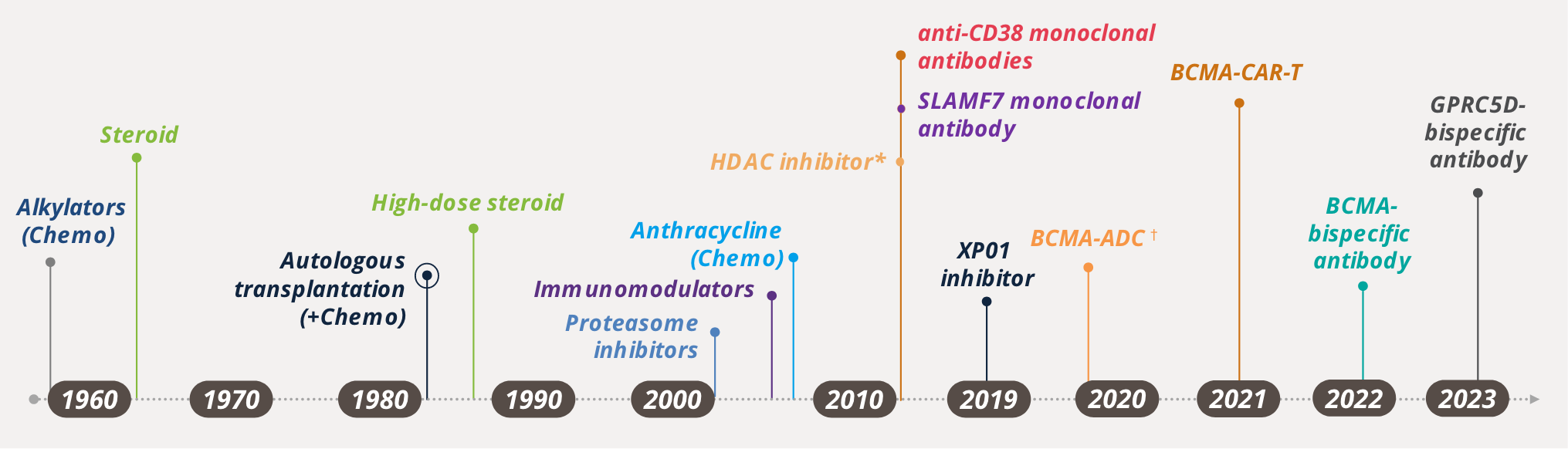
Understanding Multiple Myeloma (MM): Quick Insights Into Diagnosis and Treatment
IMWG Diagnostic Criteria for MM10
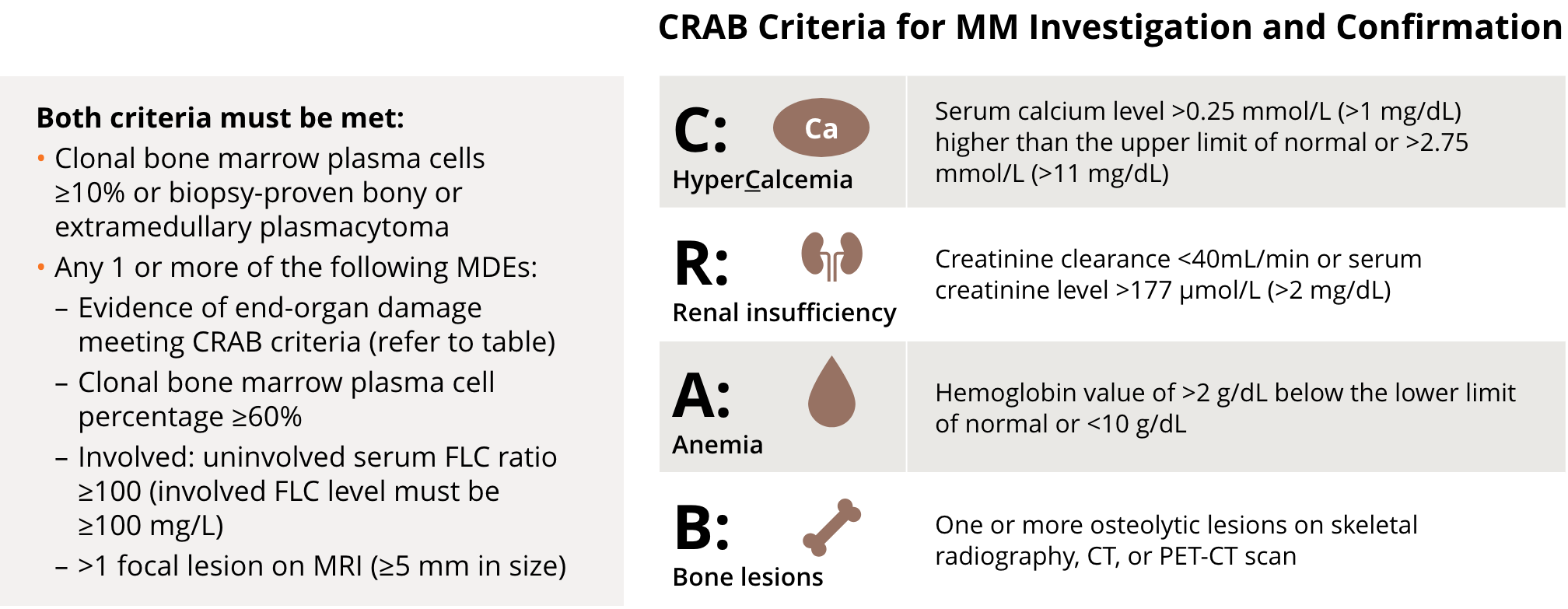
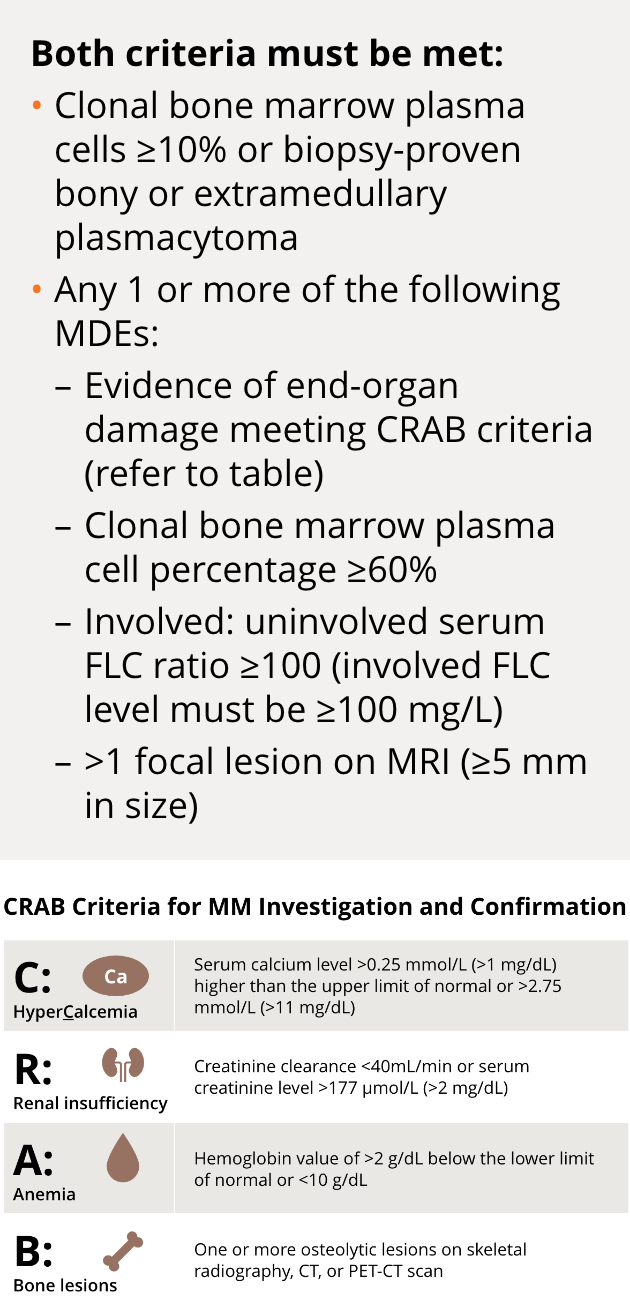
The CRAB criteria for detection of MM assess patients based on the presence of 4 parameters: hypercalcemia, renal impairment, anemia, and bone lesions.
Increased awareness of clinical features of MM, including its presentation as bone pain, may lead to early recognition and testing of MM in primary care—which could potentially accelerate disease diagnosis and timely treatment.11
CT, computed tomography; FLC, free light chain; IMWG, International Myeloma Working Group; MDE, myeloma-defining event; MRI, magnetic resonance imaging; PET-CT, positron emission tomography-computed
tomography.
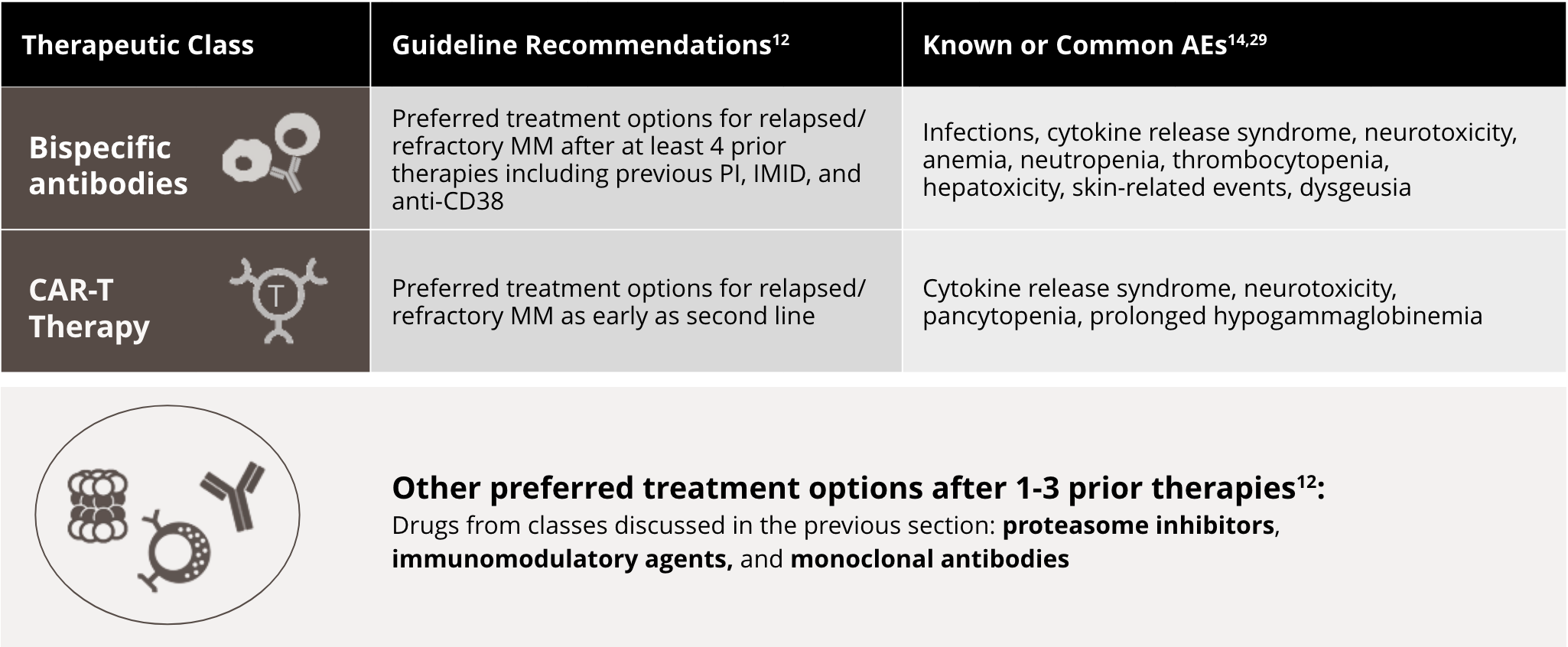
Treatment of Newly Diagnosed MM12

- One of the first steps in evaluating newly diagnosed patients with MM is to determine whether they are candidates for high-dose therapy and transplant, based on age and comorbidities. However, it should be noted that advanced age and renal dysfunction are not absolute contraindications to transplant. Therefore, referral to an HCT center to assess whether the patient is eligible for HCT is important
- ASCT has demonstrated survival benefit in multiple clinical trials and is currently considered for all newly diagnosed transplant-eligible patients
- The treatment regimen includes induction therapy followed by HDT with ASCT
- For transplant-ineligible patients, induction therapy that incorporates combinations with novel agents may be considered
- Maintenance/consolidation therapy has been demonstrated to confer clinical benefit for transplant recipients and transplant-ineligible patients in some trials
- According to the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Multiple Myeloma, the primary myeloma treatment may include use of bisphosphonates or of denosumab plus supportive care treatment as indicated
ASCT, autologous stem cell transplant; HCT, hematopoietic cell transplantation; HDT, high-dose therapy; NCCN, National Comprehensive Cancer Network.
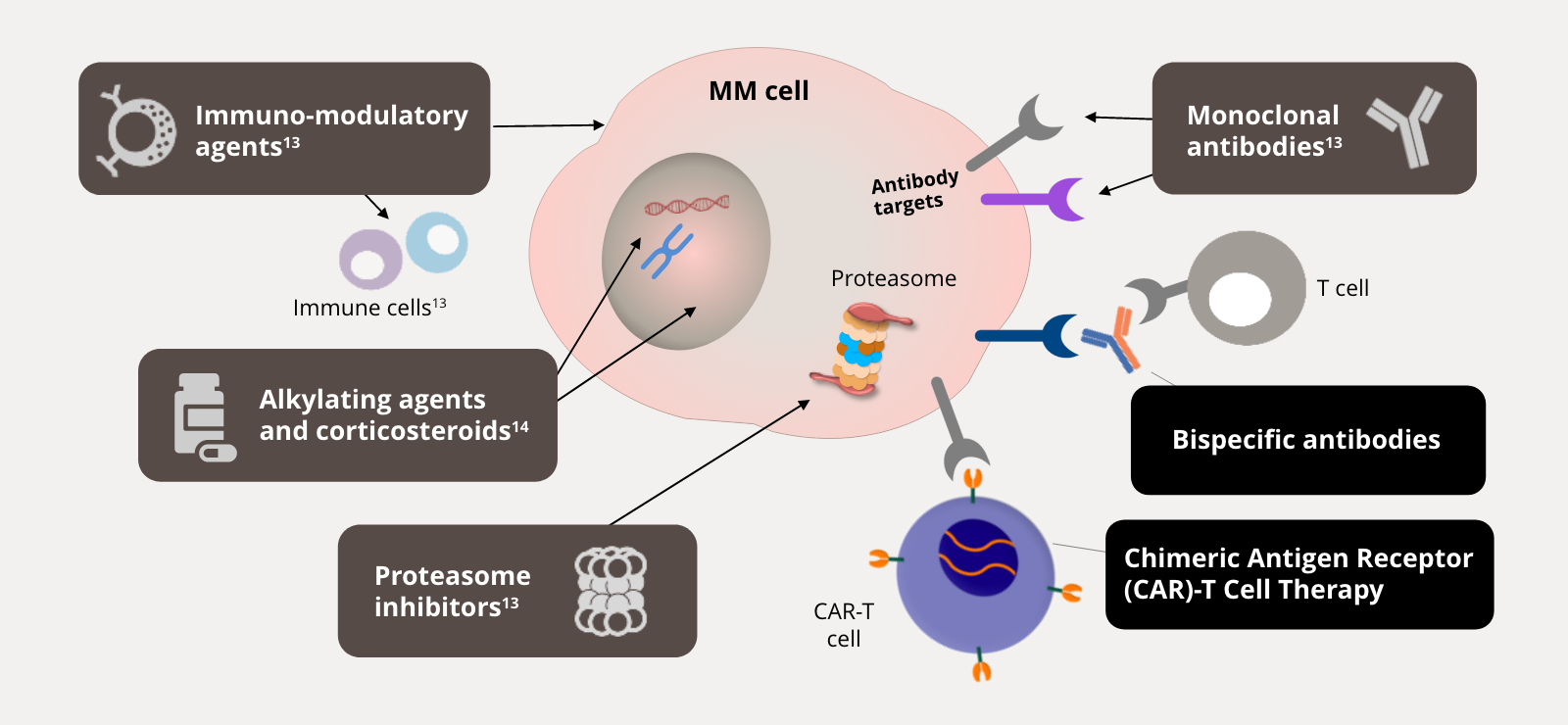
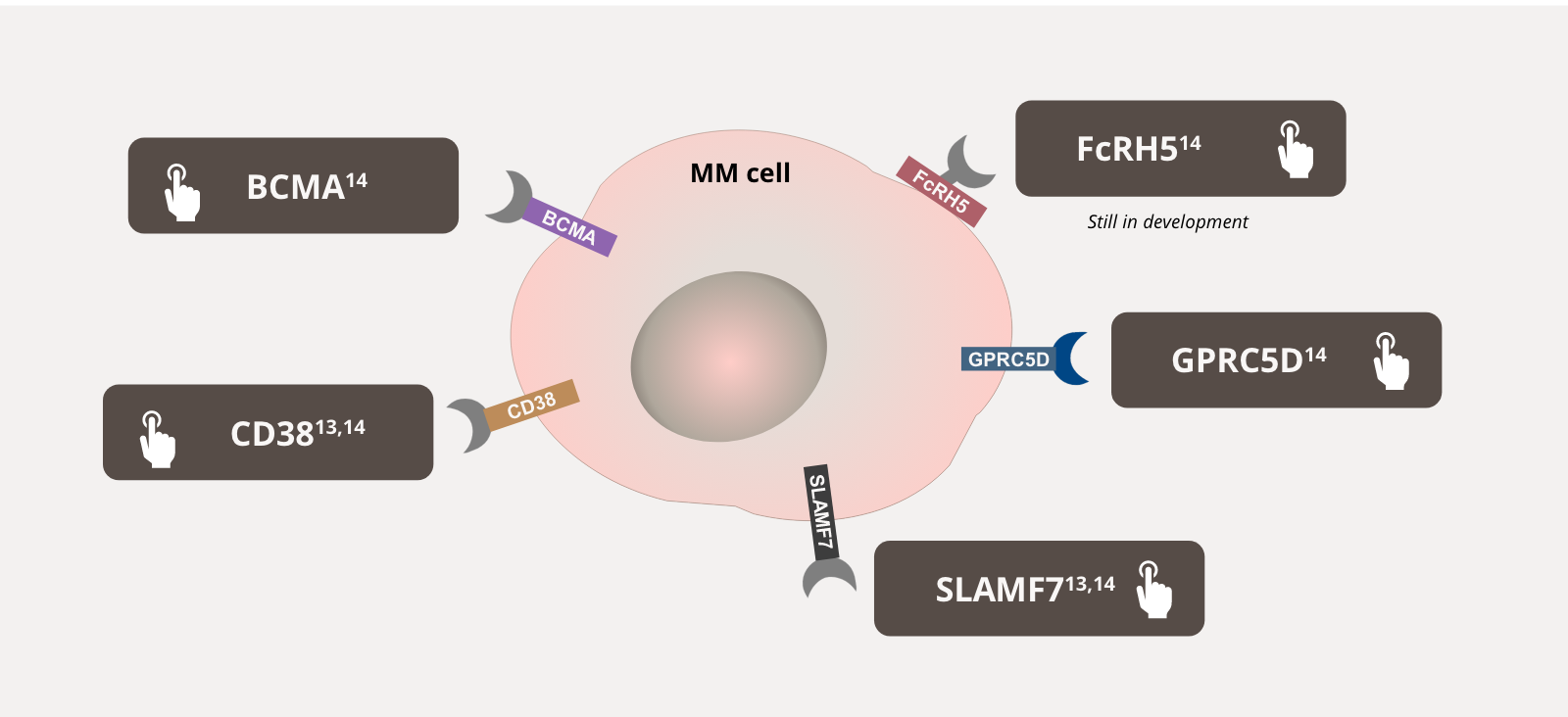
Treatment Classes for Patients with Newly Diagnosed MM
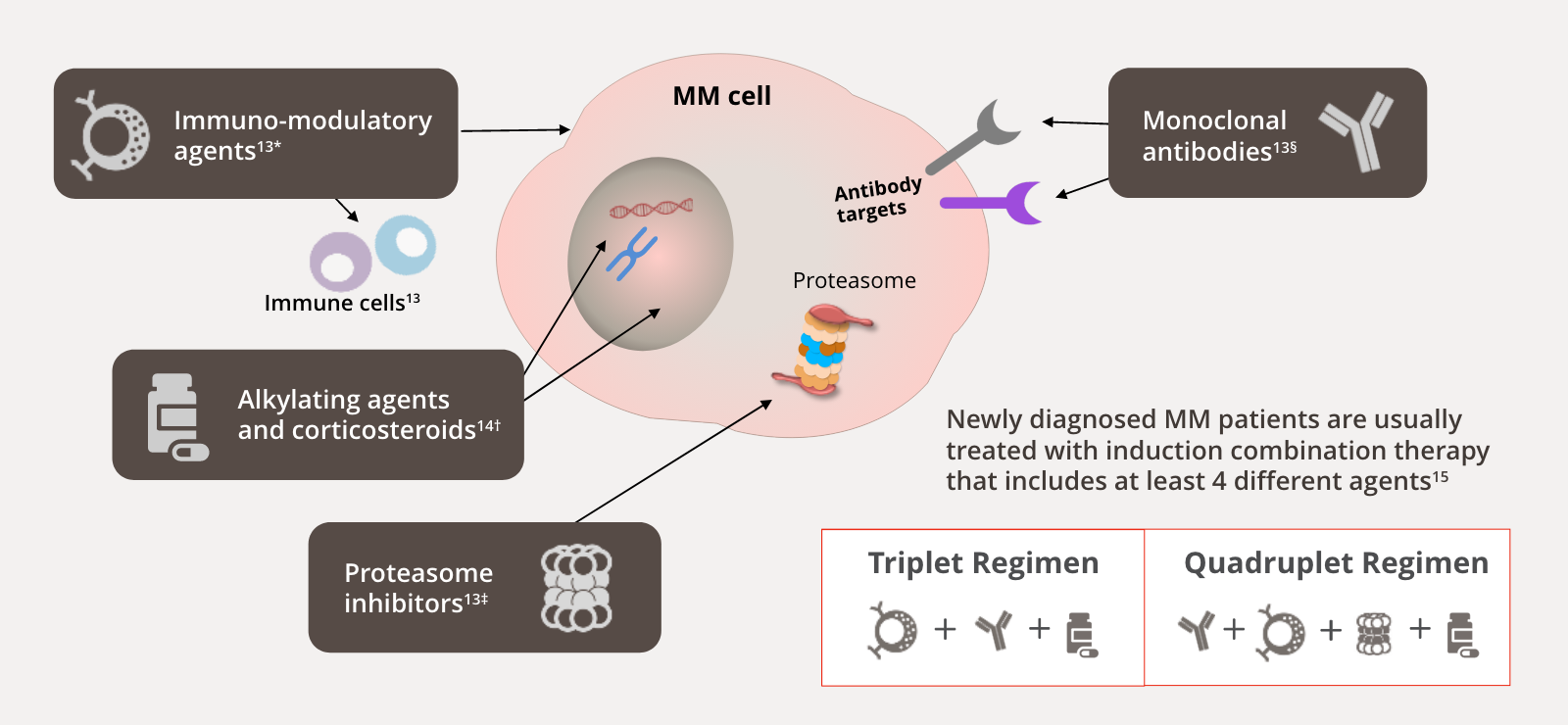
Immuno-modulatory agents have multiple anti-myeloma properties including immune modulation, anti-angiogenic, anti-inflammatory, and anti-proliferative effects. They bind to cereblon, an adaptor subunit of the E3 ubiquitin ligase.
Alkylating agents work by breaking the double strand of DNA, leading to apoptosis, corticosteroids induce apoptosis in MM cells either by transactivation of glucocorticoid response elements, phosphorylation of RAFTK (Pyk2), or transrepression of NF-Kappa B, but its exact mechanism of action is still unknown.
Proteasome inhibitors target the ubiquitin–proteasome system responsible for the degradation of intracellular proteins and the maintenance of cellular protein homeostasis. Inhibition of this system leads to cell-cycle arrest, promotion of apoptosis, and disruption of the stress response.
Monoclonal antibodies induce cell death via several mechanisms, including Fc-dependent effector mechanisms, complement-dependent cytotoxicity, and antibody-dependent cellular phagocytosis.
DNA, deoxyribonucleic acid; E3, estriol; Fc, fragment crystallizable; NF-Kappa B, nuclear factor kappa B; Pyk2, proline-rich tyrosine kinase 2; RAFTK, related adhesion focal tyrosine kinase.